To Infinity and (PRES)BYOND - The game changer for my practice



I opened my own refractive surgery practice in Perth, Australia in 2019, and when getting started I was mostly performing LASIK in pre-presbyopic patients. Perth is the fourth largest city in Australia but is the most competitive regarding refractive surgery. For instance, the number of centers offering lenticule extraction surgery is greater in Perth than in Sydney and Melbourne combined. To set myself apart from other centers, I saw a potential for practice building by offering solutions for presbyopia in patients without cataract, as this is a huge patient group whose special needs are currently not addressed by all clinics. My theory proved to be correct because within a few years, the latter group became a significant segment of my practice, accounting for about 35% of the total share.
Like most surgeons in Australia, I was performing refractive lens replacements (RLR) with multifocal IOL implantation to manage presbyopic patients without cataract, despite the disadvantages and risks of that approach.1 I tried a multifocal corneal approach but stopped after 9 patients because the results were far below my and my patients’ expectations.
In June 2022 I traveled to London, UK, to take the London Vision Clinic’s Forefront Refractive surgery course led by Prof. Dan Z. Reinstein and Mr Glenn Carp. My primary purpose for attending the program was my interest in augmenting my surgical portfolio for corneal refractive surgery with Lenticule Extraction (LE). The course also covered PRESBYOND from ZEISS, a corneal solution for treating presbyopic patients that differed from anything I had known before. I was intrigued by Prof Reinstein’s description of the results and benefits of PRESBYOND® and saw it as a great opportunity to meet the needs of my younger presbyopic patients without cataract seeking spectacle independence and to expand my practice.


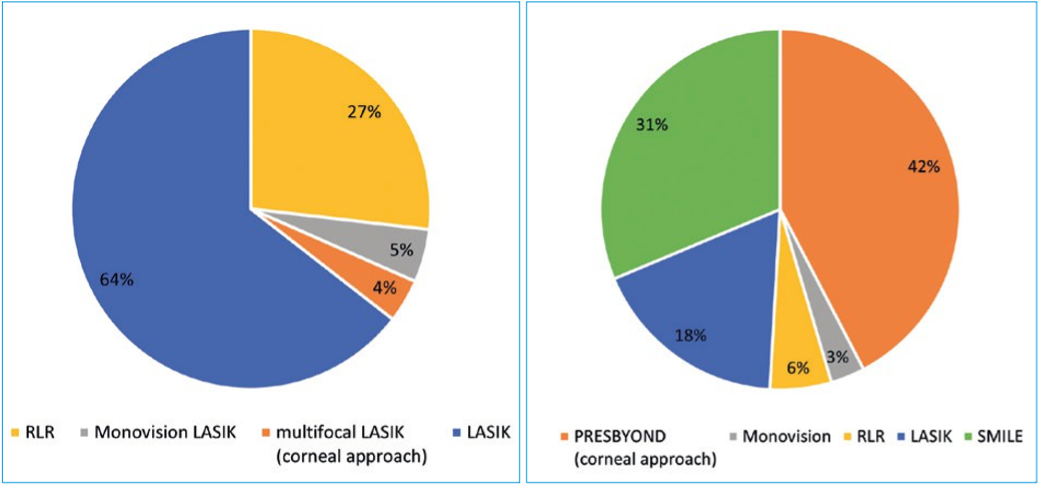
Figure: Surgical volume distribution
PRESBYOND® is a software for planning a customized binocular LASIK procedure to both manage presbyopia and correct refractive error. It increases the depth of field by inducing a controlled amount of spherical aberration and creating a micro-anisometropia (≤1.5 D), the latter being well-tolerated by most patients. Studies have shown that up to 97% of presbyopic patients tolerate the micro- anisometropia.2 PRESBYOND® gives patients a continuous range of quality vision from near to far, has the accuracy of a laser refractive procedure, and avoids the drawbacks that accompany other methods used for surgical management of presbyopia like glare and haloes at nighttime. Importantly, patients treated with PRESBYOND® maintain stereoacuity and contrast sensitivity.
My personal success story
I began performing PRESBYOND® in September 2022, and it did not take long before it proved itself to be a valuable addition to my surgical armamentarium. Not only did the outcomes I was achieving show me that by implementing PRESBYOND® I had made the right decision for my patients, but reviewing my surgical volumes and center’s revenues, I knew that I had also made a fantastic business decision for my practice.
I recently analyzed visual acuity outcomes for my first 41 PRESBYOND® cases that comprised a mix of myopic and hyperopic patients. Subjective reports showed most patients were spectacle independent. No patient needed reading glasses, although some patients said they benefited from wearing glasses at certain times, especially for night driving. No patient lost ≥2 lines CDVA and no one was unhappy.
The analysis of my caseload and case distribution data showed that my total surgical volume increased more than 41% comparing the same 9-month period (Sept – May) from before and after I implemented both PRESBYOND® and LE with SMILE® (Figure).
Although both PRESBYOND® and SMILE® contributed to the increase, PRESBYOND® was the primary driver, largely accounting for a more than doubling of my total presbyopic treatments, which went from 82 to 166. Furthermore, after introducing PRESBYOND®, treatment for presbyopia in patients without cataract came to represent a majority of my procedures, accounting for 51% of my steadily growing clinic volume. The number of RLR procedures I performed dropped drastically since PRESBYOND® has become my first choice for younger presbyopic patients without cataract. Now I only perform RLR in occasional cases when a specific patient is not suitable for a LASIK procedure.
Equipment, training and marketing – What it took to get started
When I returned from Prof Reinstein’s course, I sold my excimer laser and ordered both the MEL® 90 excimer laser and the VISUMAX® 800 femtosecond laser.
In addition to having the necessary equipment for PRESBYOND®, it is also very important for surgeons to prepare themselves and their staff and to adapt the clinic’s workflow accordingly. While waiting for the delivery of my new lasers, my staff and I worked tirelessly to prepare for successful PRESBYOND® implementation. Attending Prof Reinstein’s course was essential for giving me the necessary foundation. Then my staff and I watched and rewatched video course material, and my optometrist and I practiced to both perfect our specific refraction skills needed for PRESBYOND®, and to refine our counseling conversations for potential patients.
Surgeons who are performing LASIK will find that the learning curve for the procedure itself is very short, since it is basically a LASIK procedure. In my opinion, however, one must first have a thorough understanding of the theory and working principle of PRESBYOND® along with knowledge of the components of the screening evaluation and preoperative workup that are essential for proper patient selection and surgical planning. Most patients are suitable candidates for PRESBYOND®, and accurate preoperative measurements are critical for customized planning of the ablation that is best for all individuals.
It had been suggested to perform at least 50 LASIK procedures with the MEL 90 from ZEISS to achieve very good clinical outcomes with LASIK patients and if necessary fine tune nomograms before beginning to use the laser for PRESBYOND®. Because I was obtaining such predictably accurate outcomes with MEL® 90 for my LASIK patients, I was able to introduce PRESBYOND® within 1 month.
Initially, I was marketing PRESBYOND® to consumers and referring eye care practitioners quite extensively. I recommend that surgeons starting out with ZEISS PRESBYOND do the same to set their practice apart from others. I had articles and advertisements placed in local newspapers and held continuing professional development meetings for optometrists and general ophthalmologists. During those meetings I had patients share their experience because I thought their success stories would be more convincing than my lecturing. I also offered PRESBYOND® to optometrists and general practitioners, confident that these practitioners would become satisfied patients and a lifelong source of referrals. In fact, my practice benefits from a wide referral base, and is now the prime center in Perth for surgical management of presbyopia. My success with PRESBYOND® now draws patients to my practice through word-of-mouth referrals, and our need to advertise the procedure has significantly decreased.
Conclusion
Addressing the needs of presbyopic patients has definitely been one of the best decisions for my practice. However, as reflected by my surgical volume data, the real game changer has been the switch from my original RLR approach to the corneal approach with PRESBYOND® as my procedure of choice for this large pool of potential patients. The functional results I am achieving with PRESBYOND® speak for themselves in confirming that it is a safe and effective procedure for managing presbyopia in patients with myopia4, hyperopia5, and emmetropia2. Moreover, the dramatic effect that “word of mouth” referrals are having on my practice growth is testament to the high level of patient satisfaction.
The trust in my gut feeling and the commitment of my team certainly had important roles in leading me along the path to “Infinity and PRESBYOND®”. But, implementing PRESBYOND® and being successful also involves investment and effort. The MEL® 90 laser and refractive workplace station with the PRESBYOND software from ZEISS are requisite. In addition, the surgeon and staff must become well-versed in the principles of PRESBYOND®, components of the screening evaluation, preoperative work-up, and elements of proper patient education. In closing, I hope that my experience with PRESBYOND® might motivate its adoption by other surgeons because I firmly believe that just like me, they will find benefit both for themselves and their patients.



Lourens van Zyl, MBChB is medical director and founder of the Crystal Eye and Laser Centre, Perth, Australia. He is a paid consultant to Carl Zeiss Meditec.
References
1. Alvarado-Villacorta R, Hernandez-Quintela E, De La Torre-Gonzalez E, Loza Munárriz C, Martinez- Zapata MJ. Surgical interventions for presbyopia (Protocol). Cochrane Database of Systematic Reviews. 2023, Issue 3. Art. No.: CD015711.
2. Reinstein DZ, Carp GI, Archer TJ, Gobbe M. LASIK for the correction of presbyopia in emmetropic patients using aspheric ablation profiles and a micro-monovision protocol with the Carl Zeiss Meditec MEL80 and VisuMax. J Refract Surg. 2012; 28:531-541.
3. Brar S, Sute SS, Bagare SN, Ganesh S. Functional outcomes and reading speeds following PRESBYOND LBV using nonlinear aspheric ablation profiles combined with micro-monovision. J Ophthalmol. 2021;2021:2957443.
4. Reinstein DZ, Archer TJ, Gobbe M. LASIK for Myopic Astigmatism and presbyopia using onlinear aspheric micro-monovision with the Carl Zeiss Meditec MEL 80 platform. J Refract Surg. 2011;27(1):23-37.
5. Reinstein DZ, Couch DG, Archer TJ. LASIK for hyperopic astigmatism and presbyopia using micromonovision with the Carl Zeiss Meditec MEL80 platform. J Refract Surg. 2009;25(1):37-58.





