News|Articles|November 1, 2023
Presbyopia correction in cataract surgery: Maximizing success and satisfaction with the new AT ELANA 841P IOL
Author(s)MUDr. Peter Mojžiš, Ph.D., FEBO
Advertisement
When the ESCRS Clinical Trends Survey was first conducted in 2016 and in every subsequent year, trifocal IOLs have ranked as the type of technology used most often by cataract surgeons for patients seeking presbyopia correction.1 Looking back over the history of presbyopia-correcting IOLs coming onto the market, I believe that the introduction of the AT LISA® tri family of hydrophilic lenses from ZEISS was a huge advance considering the clinical outcomes achieved and corresponding high level of patient satisfaction.2,3
In September 2023, ZEISS extended its portfolio of trifocal IOLs with the launch of the AT ELANA® 841P IOL, a single- piece hydrophobic acrylic implant that offers the benefits of two time-tested technologies (Figure 1).
First, the AT ELANA is based on the optical design of the single- piece, four point-haptic AT LISA tri 839MP. Building on the clinical performance of the AT LISA tri 839MP that is proven by results reported in over 170 peer-reviewed papers, the optical design of the AT ELANA features a further optimization of the diffractive structure to improve near-to-intermediate visual acuity (VA) without compromising distance VA.* 2,3 Second, the AT ELANA is built with the same hydrophobic acrylic and C-loop platform found in the CT LUCIA 621P IOL, which are features that confer ease and stability of intraocular positioning along with resistance to posterior capsule opacification (PCO).4,5
The AT ELANA in detail
The foldable AT ELANA 841P is made of a glistening-free** hydrophobic acrylic that allows for optimal image quality. This new lens is available in a wide range of powers (0.0 D to +34.0 D), and it comes fully preloaded in the easy-to-use BLUESERT™ injector that provides reliable implantation while enhancing surgical efficiency and safety by eliminating the need for IOL loading. Heparin coating*** on the surface of the AT ELANA 841P further enables controlled delivery by supporting smooth unfolding.
The ZEISS AT ELANA 841P has a spherical aberration- neutral optic, featuring diffractive rings across its entire surface. It incorporates patented SMP (smooth micro phase) manufacturing technology from ZEISS that minimizes light scattering and the related visual symptom. Increased light transmission through the optic improves overall image quality, and allocation of a higher proportion of light for near vision could explain the AT ELANA’s performance for enhancing near- to-intermediate vision while preserving far visual acuity.*
The AT ELANA 841P optic has a 360° square edge, a design that has been shown to be key for preventing PCO.6 Its step- vaulted C-loop haptics and specially designed and reinforced optic-haptic junction have been shown to maximize capsular contact, which can further reduce PCO, and serve to enable centration and maintain positional stability that are requisite for optimal visual performance with a multifocal IOL.4,5
Positive preliminary experience
I had the opportunity to implant the AT ELANA 841P before its commercial launch, and as highlighted in the following two cases, I achieved impressive outcomes in my earliest experience.
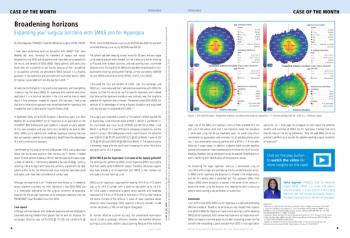
One of the first patients I implanted with the AT ELANA 841P was a 63-year-old surgeon colleague in the department of internal medicine. His complaint of decreased VA was confirmed on examination (logMAR UDVA 1.1/0.24 OD/OS; logMAR CDVA 0.24/0.16 OD/OS). He had bilateral cataracts (Grades 4/3 OD/OS) and myopia (-2.5/-0.5@122° OD, -2.75/-0.25 D@69° OS). A +20.0 D AT ELANA 841P IOL was implanted bilaterally in an uncomplicated procedure. Slit-lamp examination at 3 months postoperatively showed the IOLs were well-centered (Figure 2).
At 4 months, refraction was +0.25 D/-0.5 D@101° OD and 0.0 D/-0.25 D@92° OS; binocular uncorrected VA was logMAR -0.20 for distance, -0.18 for intermediate, and -0.08 for near. Findings from diagnostic imaging showing significant improvement in the PSF and Strehl ratio along with a decrease in ocular aberrations were consistent with the measured VA gains at all distances.
Another early patient was a retired 68-year-old gentleman who was passionate about practicing archery. He presented to our clinic with complaints about decreased blurry vision that caused him to stop participating in his favorite recreational activity. Examination showed bilateral cataracts (Grades 4/3, OD/OS) and decreased visual acuity (logMAR UDVA 0.34/0.30 OD/OS, logMAR CDVA 0.22/0.16 OD/OS). The patient underwent bilateral cataract surgery with implantation of AT ELANA 841P IOLs (+20.0/+20.5 D OD/OS). At 1 month, his refraction was 0 D/-0.50 D@138° OD and 0 D/-0.75 D@15° OS. Binocular uncorrected logMAR VA was -0.14 for distance, -0.02 for intermediate, and 0.16 for near. His VA results were consistent with assessments of visual quality, including point spread function (PSF) and Strehl ratio. Importantly and rewardingly, the patient was extremely happy with the outcome that allowed him to return to archery.
Patient-reported outcomes
Although results from the ESCRS Clinical Trends surveys show that use of presbyopia-correcting IOLs has been increasing steadily, these premium IOLs are still being implanted in a small minority of cases.1 Perhaps greater confidence that they can achieve satisfied patients might make surgeons more comfortable offering presbyopia-correcting IOLs.
Anecdotal feedback from the patients I implanted with the AT ELANA 841P indicates they are consistently happy with their outcomes. However, we have been conducting a more formal investigation of visual function using the patient-reported Catquest-9SF questionnaire, and the findings confirm my anecdotal impression (Figure 3).
Analyses of responses from an early series of 10 patients showed they were uniformly dissatisfied with their sight preoperatively and reported difficulty in everyday life because of their reduced vision. In contrast, at 3 months after surgery, all of the patients were satisfied with their sight and had no difficulty in everyday life because of their sight or when performing any of the seven vision-related tasks listed in the questionnaire.
Conclusion
My early experience with the new trifocal AT ELANA 841P has been outstanding. Overall my patients have achieved excellent visual acuity for near, intermediate, and far distances, and importantly, they have been consistently happy with their outcomes and enthusiastic about wanting to recommend the lens to their family and friends.
I would like to make my colleagues aware that with the introduction of the AT ELANA 841P, trifocal IOL technology from ZEISS is available on two distinct platforms. Therefore, regardless of their personal preference for lens biomaterial, all cataract surgeons now have the opportunity to satisfy their patients seeking presbyopia correction with clinically proven technology.
* In photopic conditions in virtual implantations and optical bench tests.
** Grade 1 (traces) or better for 85% of the patients up to and including 12 months according to Christiansen scale and based on internal clinical trial outcomes and on published clinical data.
*** Fragment of heparin used in IOL surface coating with no pharmacological, immunological or metabolic action.
References
- Kohnen T, Findl O, Nuijts R, Ribeiro F, Cochener-Lamard B. ESCRS Clinical Trends Survey 2016-2021: 6-year assessment of practice patterns among society delegates. J Cataract Refract Surg. 2023;49(2):133-141.
- Mojžiš P, Majerova K, Plaza-Puche AB, Hrckova L, Alio JL. Visual outcomes of a new toric trifocal diffractive intraocular lens. J Cataract Refract Surg. 2015;41(12):2695-706.
- Mojžiš P, Kukuckova L, Majerova K, Ziak P, Piñero DP. Postoperative visual performance with a bifocal and trifocal diffractive intraocular lens during a 1-year follow-up. Int J Ophthalmol. 2017;10(10):1528-1533.
- Borkenstein AF, Borkenstein EM. Long-term clinical results and scanning electron microscopic analysis of the aspheric, hydrophobic, acrylic intraocular lens CT LUCIA 611P(Y). Clin Ophthalmol. 2018;12:1219-1227.
- Borkenstein AF, Borkenstein EM. Geometry of acrylic, hydrophobic IOLs and changes in haptic-capsular bag relationship according to compression and different well diameters: A Bench study using computed tomography. Ophthalmol Ther. 2022;11(2):711-727.
- Vyas AV, Narendran R, Bacon PJ, Apple DJ. Three-hundred-sixty degree barrier effect of a square-edged and an enhanced-edge intraocular lens on centripetal lens epithelial cell migration Two-year results. J Cataract Refract Surg. 2007;33(1):81-87
Media placement sponsored by Carl Zeiss Meditec AG
MUDr. Peter Mojžiš, Ph.D.,FEBO is Senior Lecturer in theDepartmentofOphthalmology, Third Faculty of Medicine CharlesUniversity, Prague, CzechRepublic. He is a paid consultantfor Carl Zeiss Meditec.
Newsletter
Get the essential updates shaping the future of pharma manufacturing and compliance—subscribe today to Pharmaceutical Technology and never miss a breakthrough.
Advertisement
Related Content
Advertisement

Latest CME
























Advertisement
Advertisement